
Haematology Watch, Vol.7, Issue 1.
STUDENTS’ CORNER
EVALUATION OF 100% FOETAL HAEMOGLOBIN
{kind=link}
AETIOLOGY OF 100% FOETAL HAEMOGLOBIN:
Complete absence of HbA with presence of 100% HbF is rare and a diagnostic challenge. This anomaly happens because normal perinatal F-to-A switch fails and the patient continues to synthesize foetal hemoglobin in adult life.
This occurs in seven genetic disorders:
1. deletional homozygous hereditary persistence of fetal hemoglobin (HPFH),
2. homozygous δβ-Thalassemia:
i. (delta beta) zero-Thalassaemia
ii. homozygous G gamma (A gamma delta beta) zero-Thalassaemia
3. some cases of compound heterozygosity for δβ-thalassemia and β-thalassemia
4. compound heterozygosity for deletional HPFH and heterozygous β-Thalassemia:
5. compound heterozygosity for deletional HPFH and heterozygous δβ-Thalassaemia
6. compound heterozygosity for deletional HPFH and two gene deletional α-Thalassaemia
WHAT TO DO NEXT?
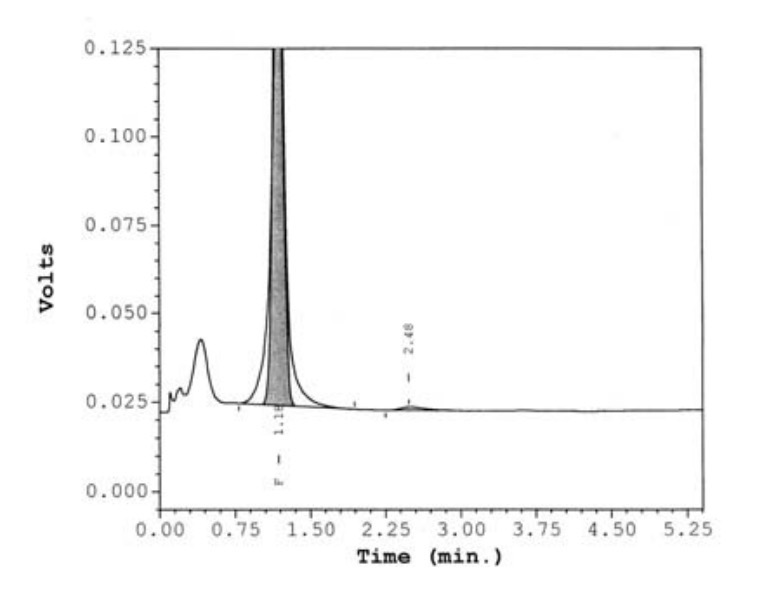
When such a picture as shown above* is seen, we have to evaluate it on following lines:
1. Verify that it is not cord blood specimen.
2. If it is an adult blood specimen:
a. Is the Hb normal? It is seen in isolated HPFH.
b. Is the patient anaemic? It is seen in other cases.
3. What do the CBC and Haemoglobin Variant Analyses of the parents tell?
4. Rest your diagnosis on the definitive test i.e. genetic testing.
These conditions can be differentiated on the basis of clinical and hematological features:
1. Deletional Homozygous HPFH:
-behaves clinically as normal, with normal red cell indices and 95 - 100% HbF.
-parents will be having heterozygous HPFH, each having normal red cell indices and 10 - 35% Hb F.
2 & 3. Homozygous δβ-Thalassaemia & Homozygous GγAγ(δβ)°-Thalassaemia:
-both varieties presents as Thalassaemia intermedia with reduced MCV & MCH, and 100% HbF.
-parents of both varieties will be Heterozygous δβ-thalassemia having CBC similar to β-Thalassaemia trait, but with high HbF (5 - 20%) & HbA2 normal or reduced.
-genetic testing will delineate more extensive genetic deletions in the latter..
4. Compound heterozygosity for δβ-Thalassaemia and heterozygous β-Thalassemia:
-presents as Thalassaemia intermedia, with ~100% HbF.
-one parent will be like heterozygous delta beta thalassaemia with high HbF (5 - 20%) & Normal or reduced HbA2 while other will be like typical β-Thalassaemia trait.
5. Compound heterozygosity for deletional HPFH and heterozygous β-Thalassemia:
-presents as mild Thalassemia intermedia, with 70 - 100% HbF.
-one parent will be like normal red cell indices and 10 - 35% Hb F while other will be having typical β-Thalassaemia trait
6. Compound heterozygosity for deletional HPFH and heterozygous δβ-Thalassaemia:
-presents as Thalassaemia intermedia, with 70 - 100% HbF.
-one parent will be having deletional heterozygous HPFH, with normal red cell indices and 10 - 35% Hb F, while other having CBC similar to β-Thalassaemia trait, but with high HbF (5 - 20%) & HbA2 normal or reduced.
7. Compound heterozygosity for homozygous deletional HPFH and two gene deletional α-Thalassaemia:
-behaves clinically as normal, but in contrast to isolated homozygous deletional HPFH, this combination has microcytosis and 100% HbF. So be careful while deciding merely on MCV & MCH to differentiate between HPFH and δβ-Thalassaemia in a population where α-Thalassaemia is prevalent!
-parents will be having heterozygous HPFH, each having normal red cell indices and 10 - 35% Hb F, along with additional features of either single α-Thalassaemia gene deletion in both or of two α-Thalassaemia gene deletions in one, affecting MCV & MCH in the latter.
-genetic testing will distinguish between HPFH and δβ-Thalassaemia in this case.
*The Image is taken from: Variant Haemoglobins, A Guide to Identification, B. Bain, p.65.