Haematology Watch, Vol 3, Issue 2.
LABORATORY HAEMATOLOGY
Correcting Total Leukocyte Count
Mehmood
To prevent false reporting is one of the responsibilities of a haematologist in a haematology laboratory. When nucleated red blood cells (NRBC) appear in circultaion, and such a sample is sent to CBC analyzers, the machine views these NRBC as white blood cells (WBC), thus falsely increasing total leukocyte count (TLC).
This type of result can be addressed by correcting TLC. This means that although the machine has taken WBC and NRBC as one type of population (i.e. nucleated one), we have to segregate their counts in order to assess true TLC, DLC, and absolute counts.
STEPS:
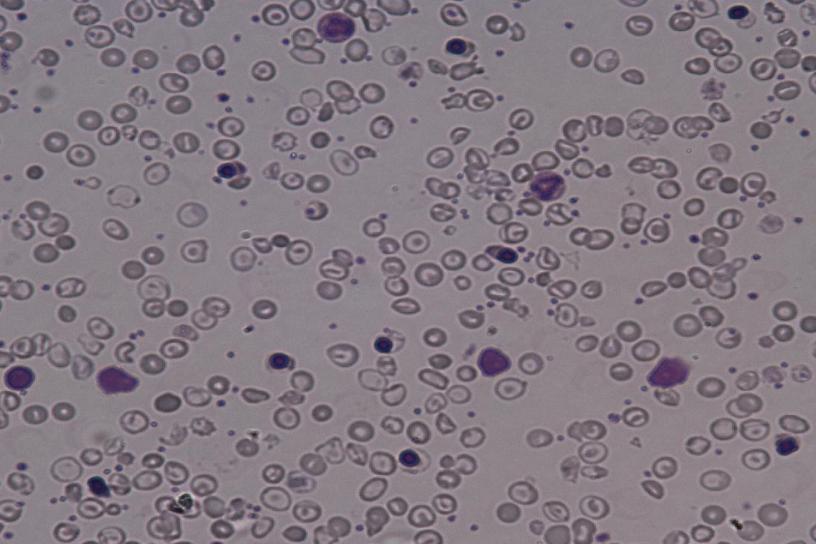
1. Observe Peripheral Blood Smear for Morphology:
- A peripheral blood cells morphology is the first step to analyze whether or not to correct TLC i.e. if occasional NRBCs are present, correcting will not yield any significant change in TLC and absolute counts. If apparently significant number of NRBCs (>5/100 WBC) are seen, proceed to step 2.
2. Perform Differential Leukocyte Count:
- It is the differential leukocyte count (DLC) that will assess the number of NRBCs.
- The number of NRBCs seen while counting WBCs for DLC are noted separately.
- Example:
DLC: NRBC:
Neutrophils: 50% 300/100 WBCs
Lymphocytes: 40%
Monocytes: 9%
Eosinophils: 1%
- This will show that 100 WBCs are counted, that NRBCs are noted separately, and that NRBCs are significantly present i.e. in this example, 3 NRBCs accompany 1 WBC.
3. Correct the Total Leukocyte Count:
- If NRBCs are significantly present, many formulae are given in literature to get true TLC:
i. Corrected TLC = TLC - [(NRBC/100) (TLC)]
ii. Corrected TLC = [100/(100+NRBC)] (TLC)
- Note that first formula is only useful if NRBC are <100/100 WBC because if NRBCs are >100/100 WBCs, the ratio will exceed TLC, thus producing an answer with a minus sign! The second formula appears to be more useful.
- Report the TLC as 'Corrected TLC'.
4. Interpret Corrected TLC:
- If the new value falls between 4000 - 10 000/uL, report as Normal, if < 4000/uL, report as leukopenia, and if > 10 000/uL, report as Leukocytosis.
5. Discover true Absolute Leukocyte Counts:
- When TLC is falsely elevated due to counting of NRBCs into nucleated cells, the absolute leukocyte counts also change.
- Correct Absolute Counts by following method:
i. Absolute Neutrophil Count (ANC)= (% of Neutrophils in DLC) (Corrected TLC)
ii. Record it as 'Corrected ANC'.
iii. Repeat the method for other leukocytes.
6. Interpret Absolute values:
- Ward personnel usually do not know values of (and "give value" to) Absolute Leukocyte Counts.
- Interpret Corrected Absolute values by giving remarks.
- Example: Corrected ALC=800/uL (Adult); Lymphopenia.
Without these steps to be followed, it is not much helpful to report that numerous NRBCs are seen per 100 WBCs. Pain of the prick of needle should be counted where cell counting counts!