
Haematology Watch, Vol.4 , Issue 1.
CASE REPORTCASE REPORT
A 15 years old male patient presented from Jhelum with a chief complaint of swollen left jaw for the last 4 months. He gave a history of fall followed by the swelling which gradually progressed, without regressing, giving him any pain, tenderness, fever, or unintentional weight loss. There was no history of discharge. Local physicians' medicines didn't help him.
Table 1: CBC parametres TLC 11000/uL TRBC 4.28 (10^6)/uL Hb 12.4 g/dL MCV 84 fL MCH 29 pg MCHC 34 g/dL PLT 37000/uL RDW-SD 45 fL ANC 7000/uL ALC 2400/uL AMC 1130/uL AEC 1000/uL ABC 20/uL |


His X-ray skull was reported as follows: A lytic lesion with multiple septations noted along with half with medial displacement of teeth. No normal bone seen in involved region. Strongly suggestive of Ameloblastoma.
His X-ray Pelvis and Ultrasonography of abadomen were unremarkable.
A CT-Scan was advised which showed:
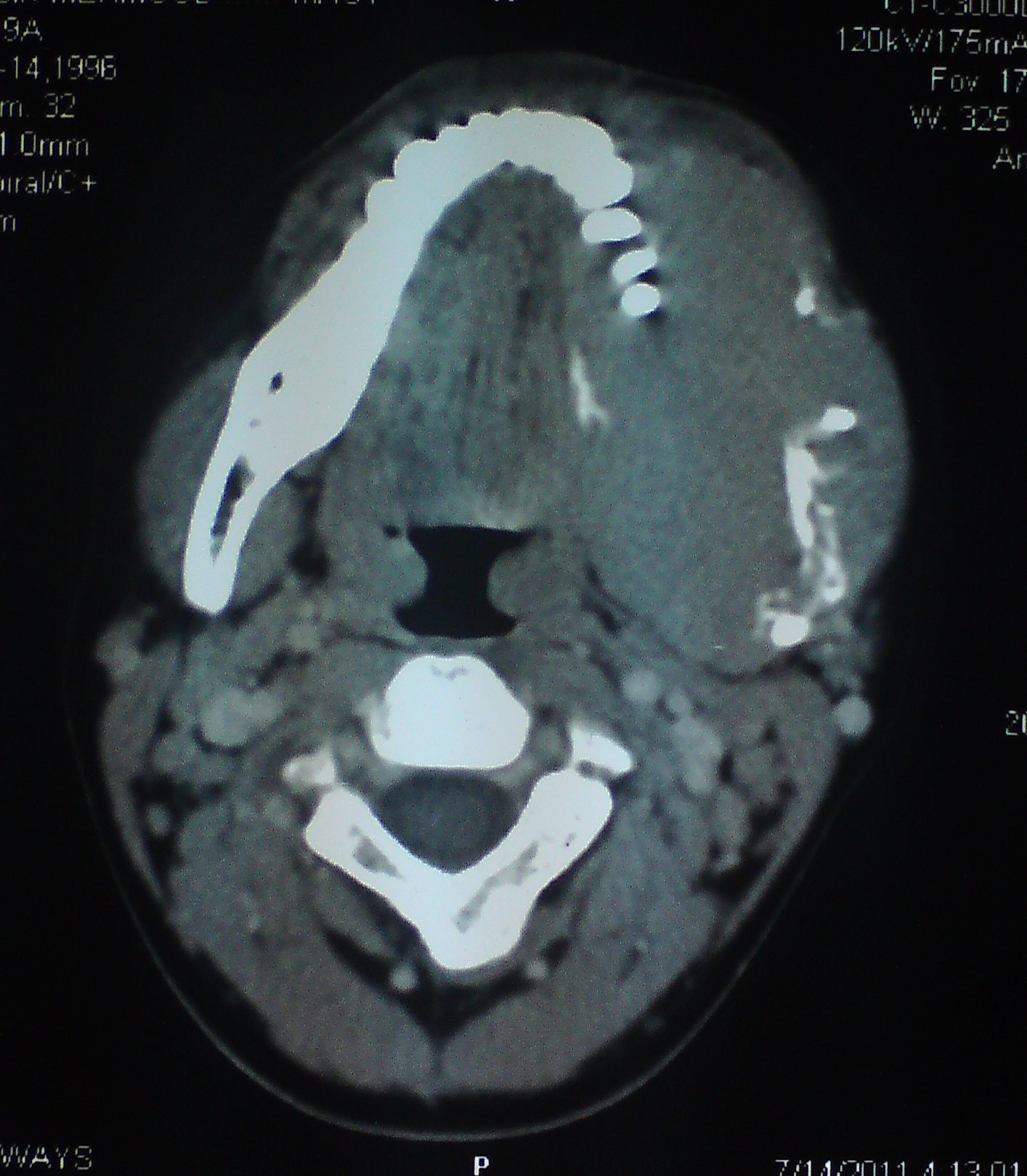
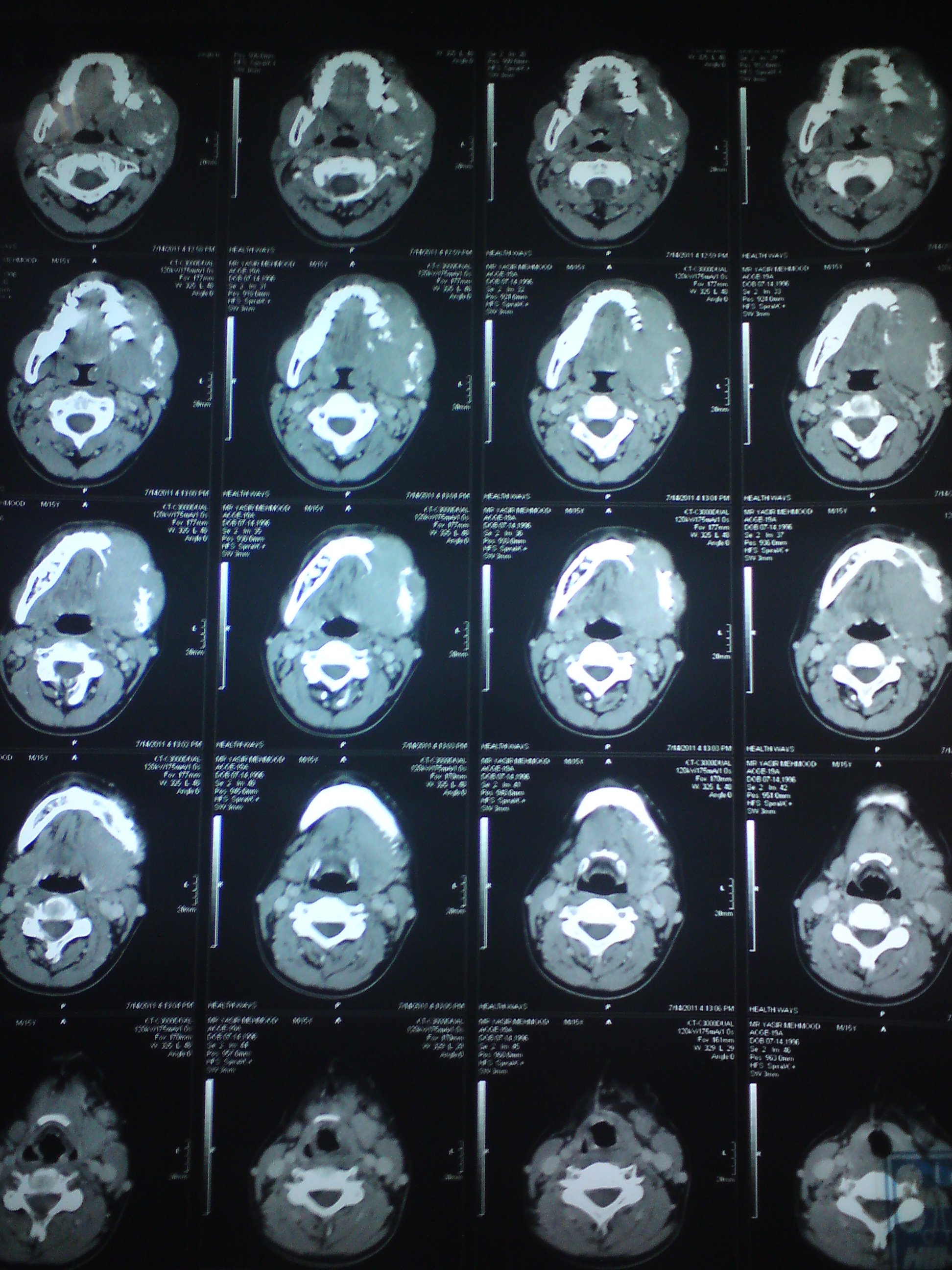
'Aggressive mass left hemimandible of odontogenic/non-odontogenic origin, with bilateral cervical lymphadenopathy at levels I and II. Biopsy correlation suggested'.
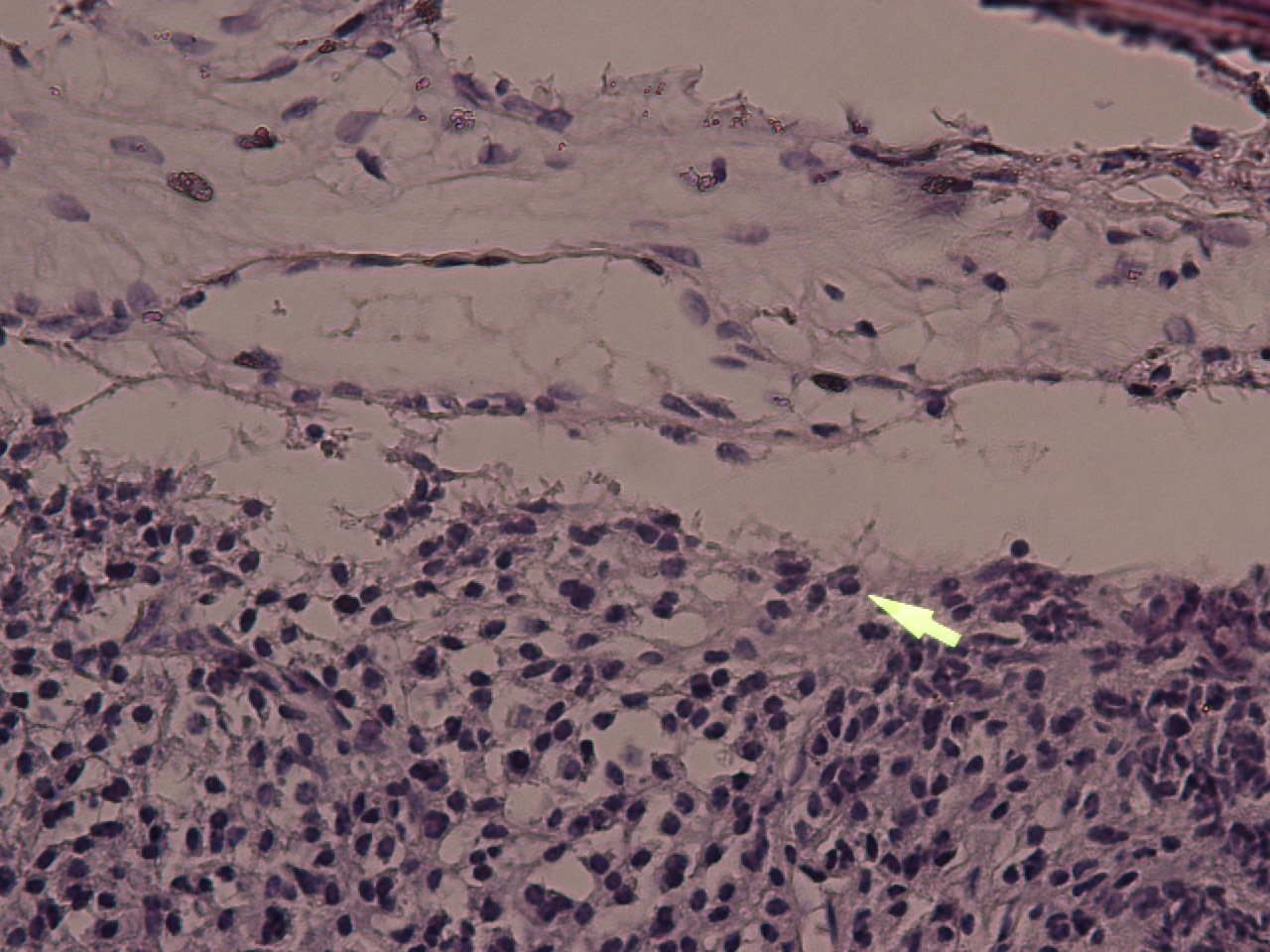
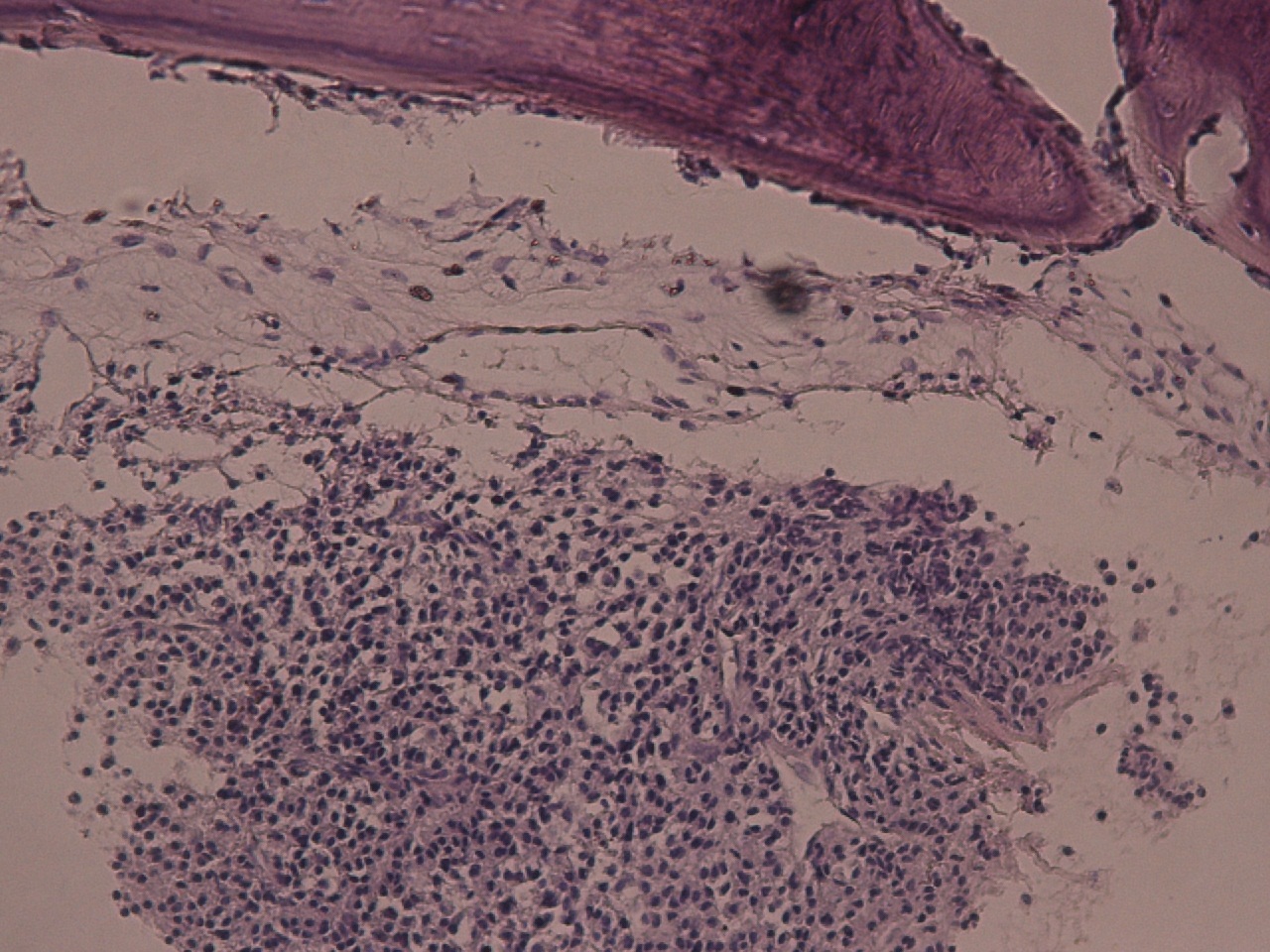
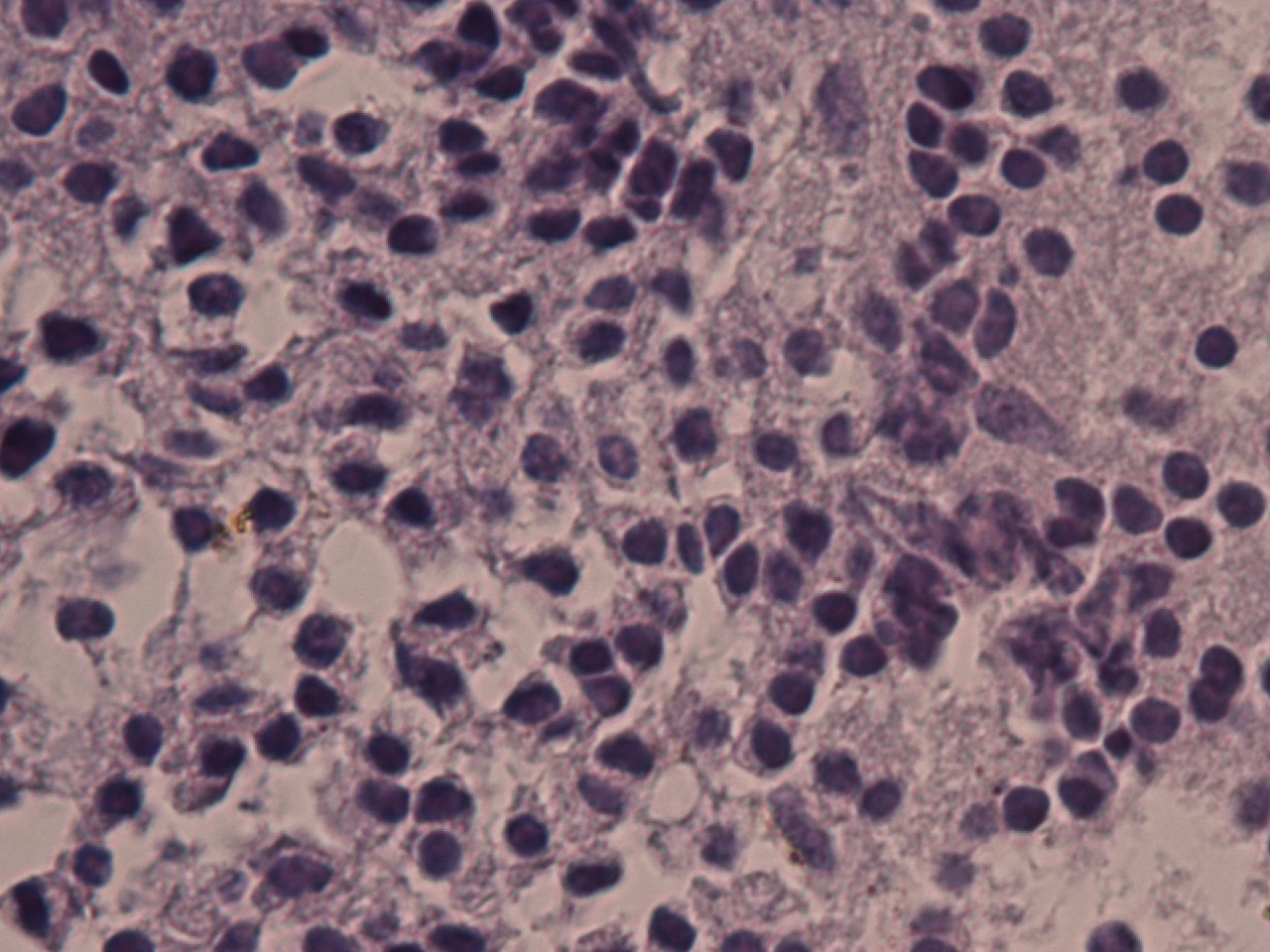
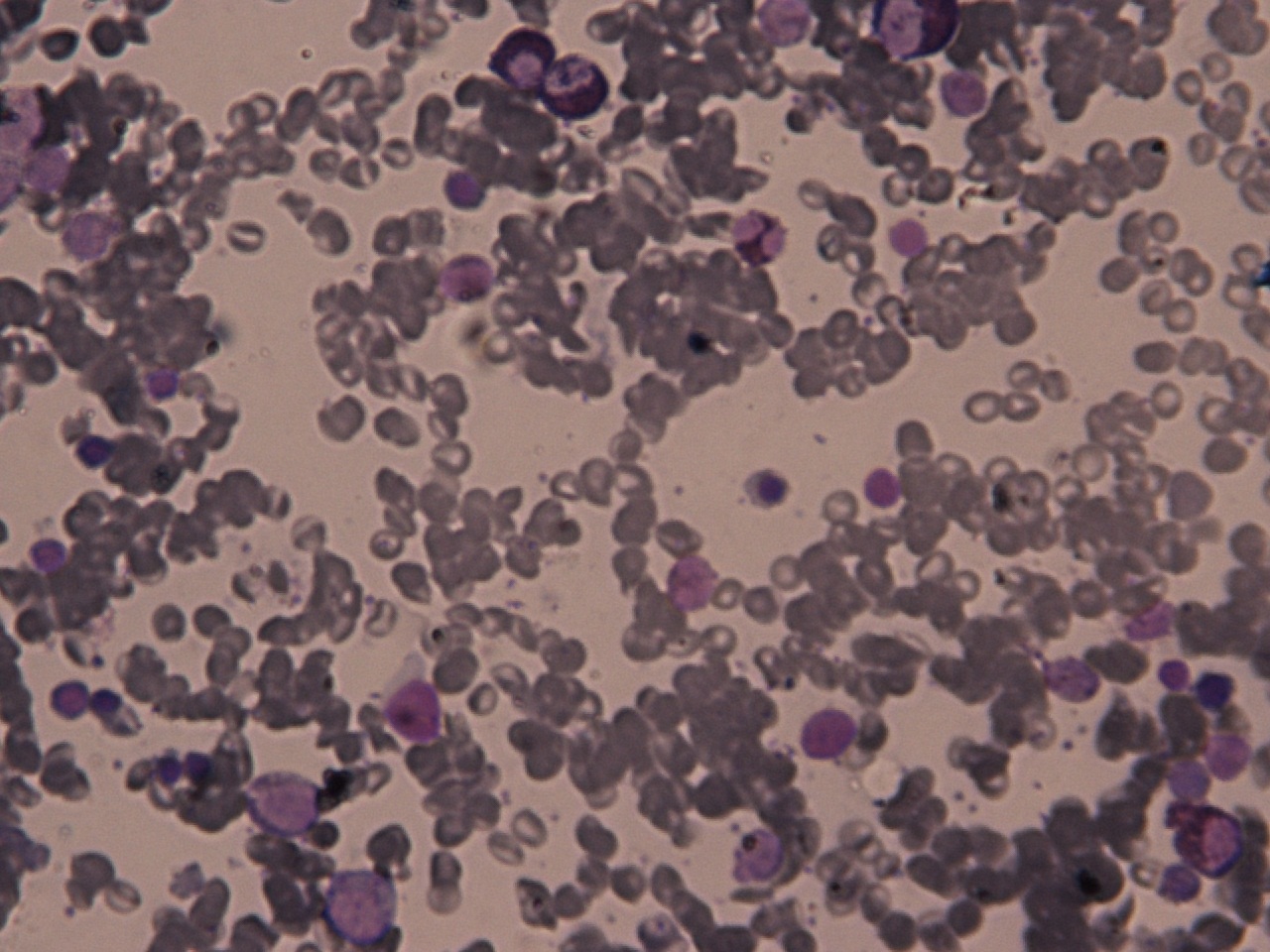
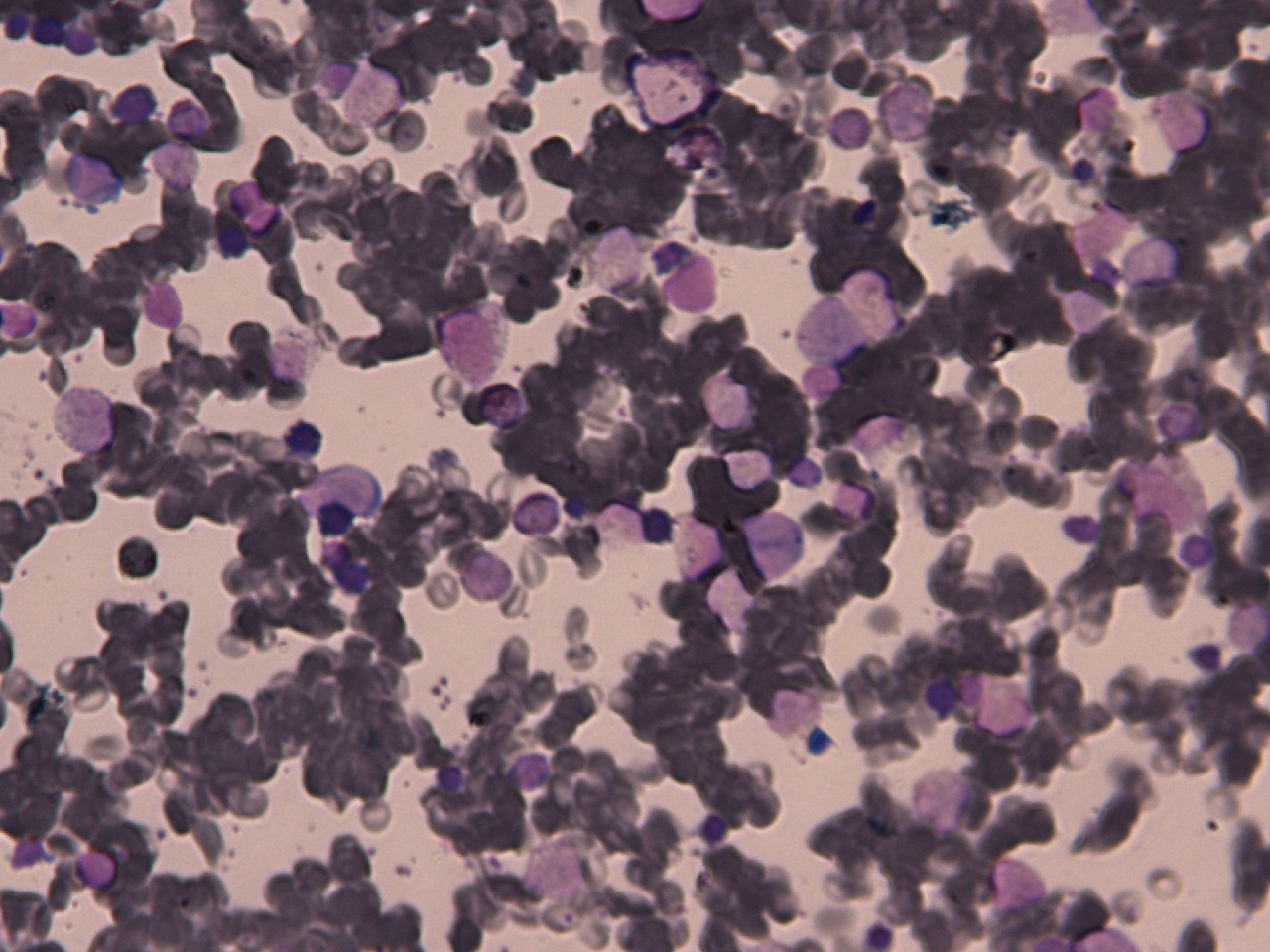
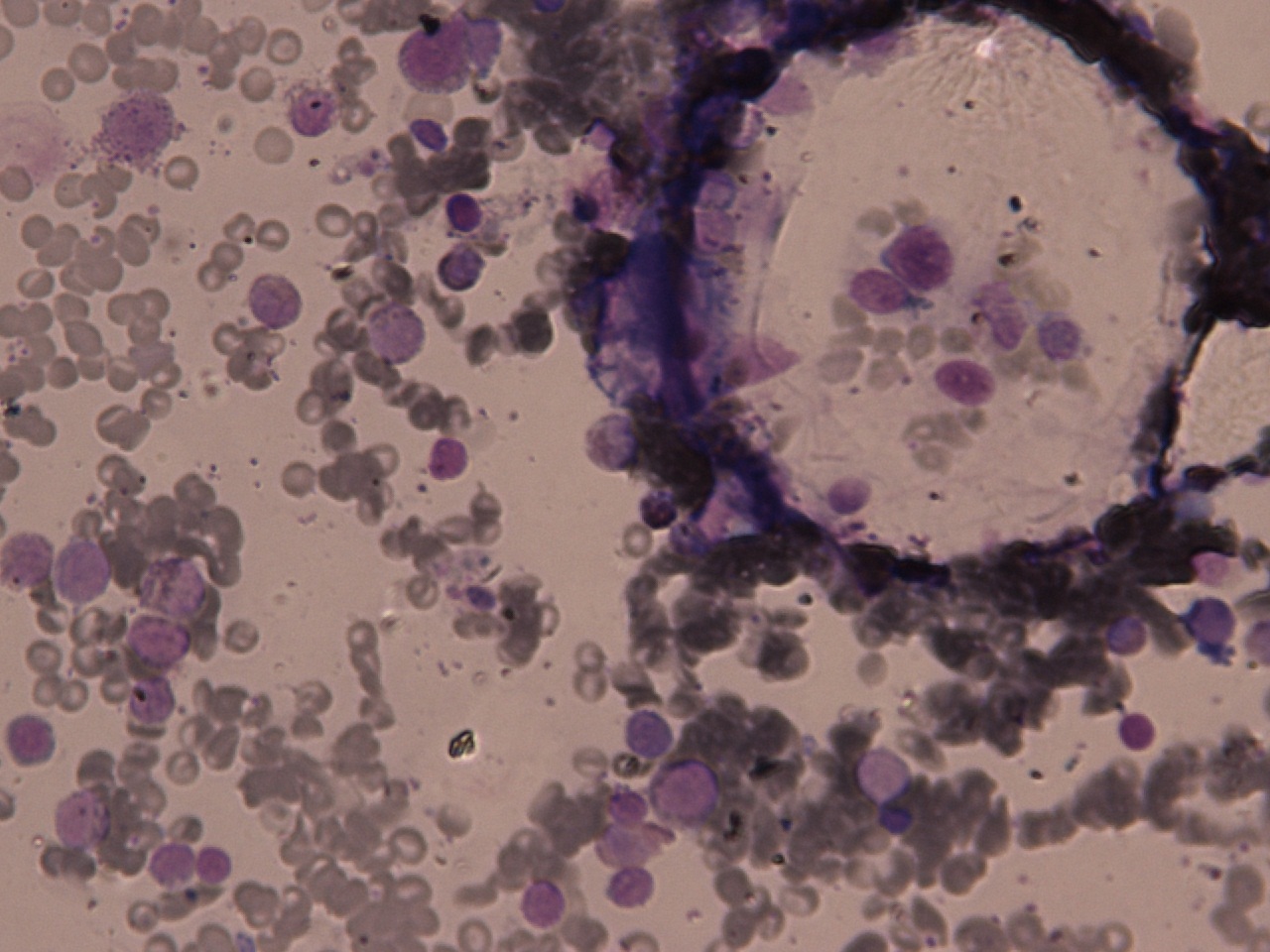
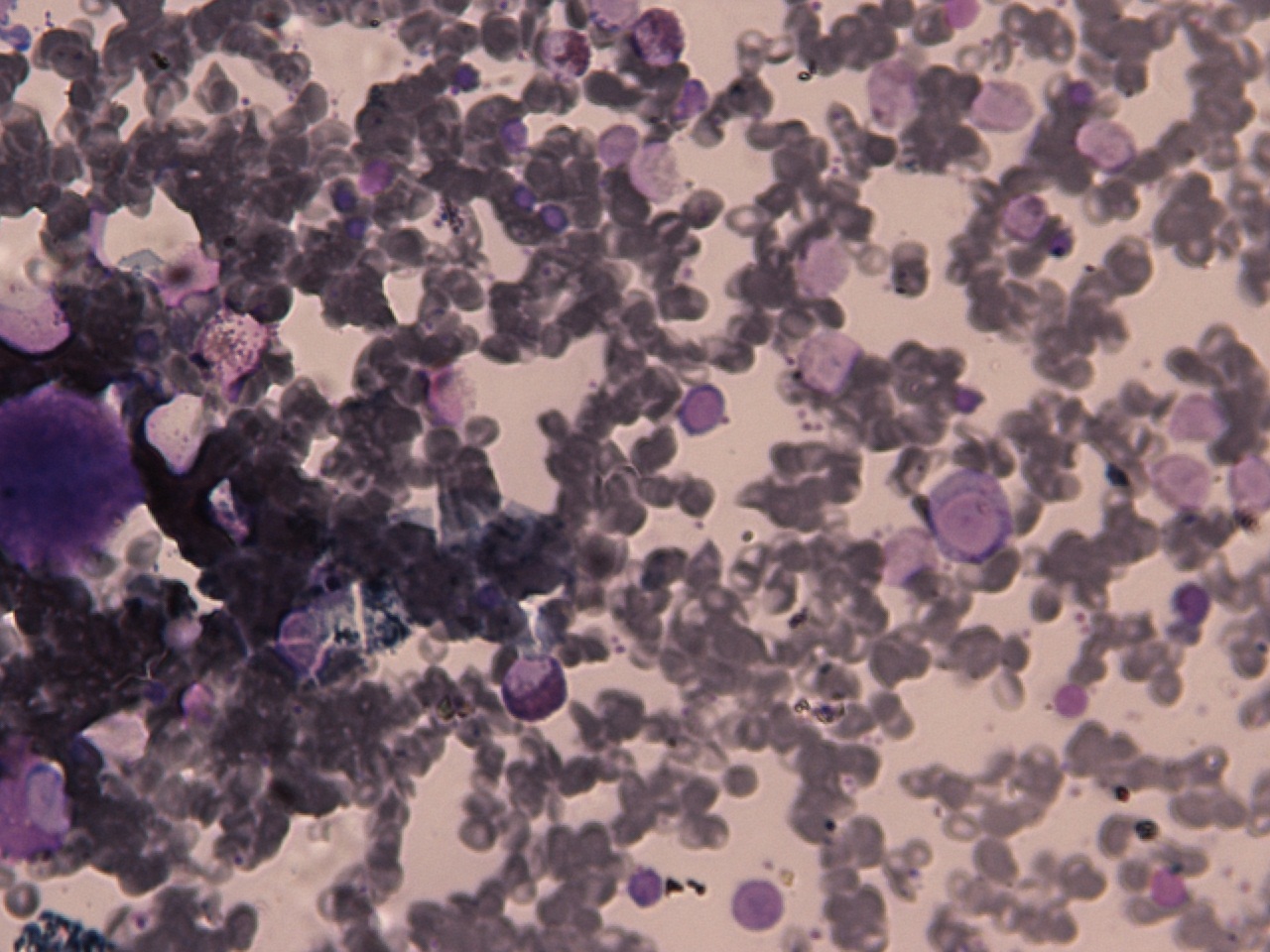
His biopsy of left mandible showed plasmacytoma.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
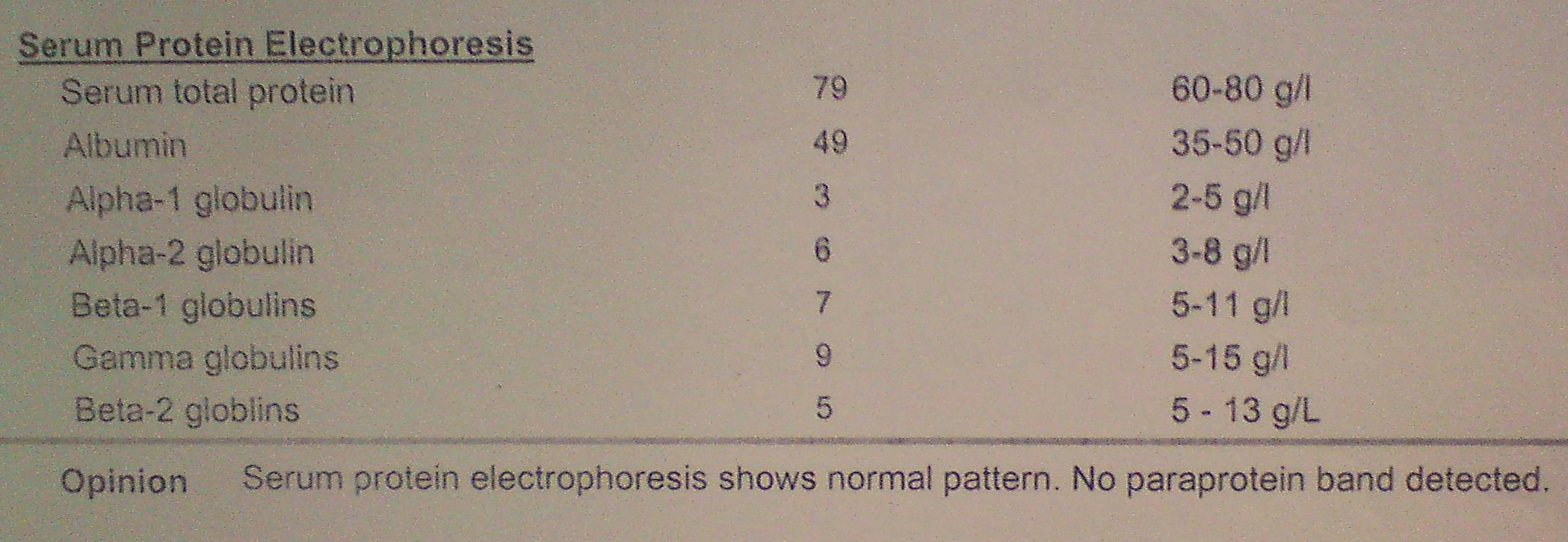
His urinary Bence-Jones proteins were absent, and protein electrophoresis revealed:
He was diagnosed as having Solitary Plasmacytoma of Bone. His radiotherapy was started which relieved his jaw swelling a lot.
DISCUSSION
Plasma cell disorders include Plasma cell myeloma (=Multiple Myeloma), Solitary Plasmacytoma of bone, Extramedullary Plasmacytoma, Monoclonal Gammopathy of Undetermined Significance (MGUS), Asymptomatic/Smouldering myeloma, Plasma cell leukaemia, Amyloidosis, Osteosclerotic myeloma (=POEMS syndrome).
Solitary Plasmacytoma is an uncommon disorder. The criteria for diagnosis includes solitary lytic bone lesion on skeletal survey, histologic confirmation of the lesion, and bone marrow plasmacytosis of <10 %. Monoclonal protein if detected is cleared after therapy. It usually affects vertebral column. In our patient the site was jaw which is rare.
In patients with low levels of paraprotein, immunofixation should be done to detect presence of small amounts which hide in the gamma globulin spike on protein electrophoresis. In our patient, it could not be done due to non-availability of the patient.